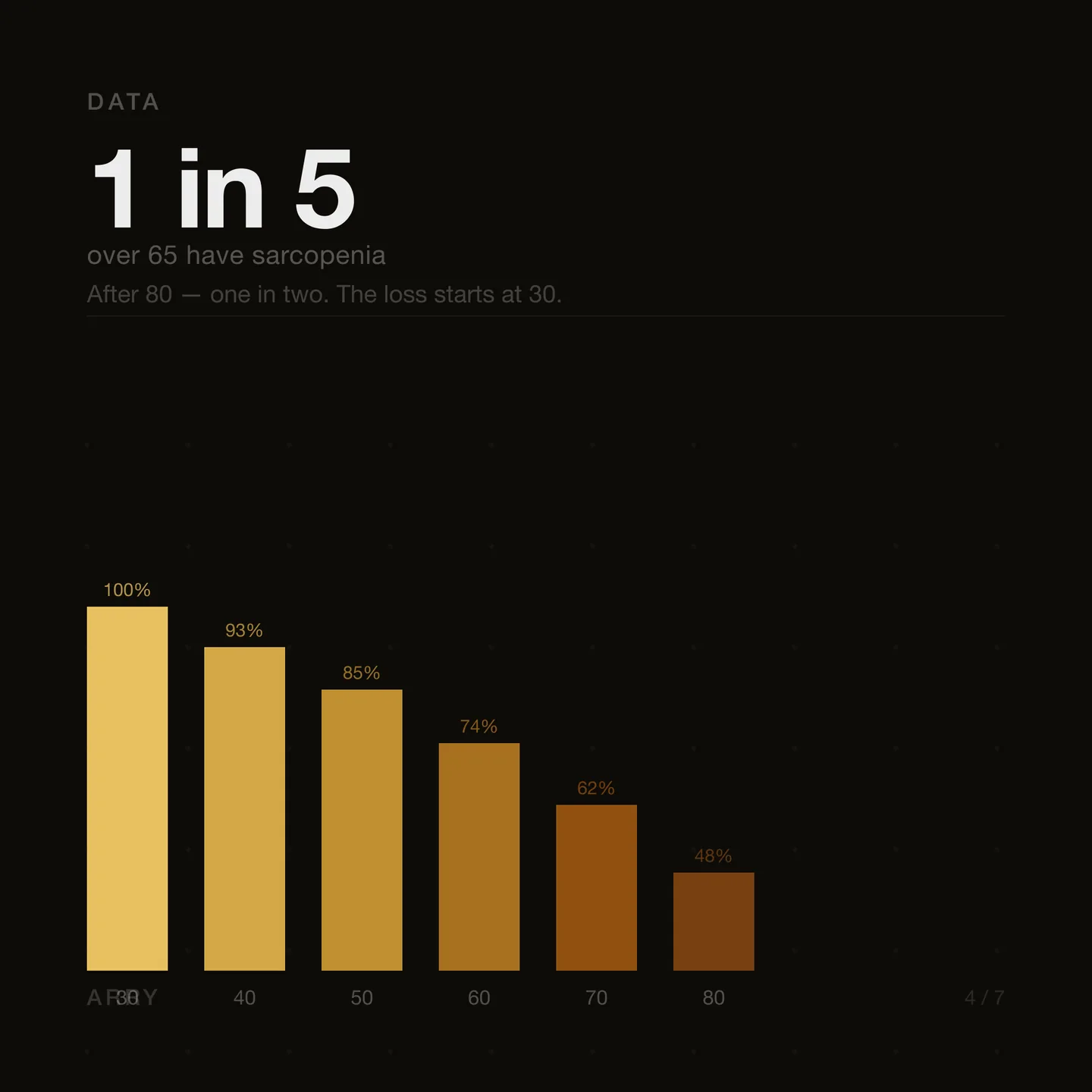
After 30, muscle mass begins declining at roughly 3–8% per decade. After 60, the rate accelerates. By 80, a person without resistance training loses up to 40% of peak muscle volume. The process is called sarcopenia — and it progresses slowly enough to go unnoticed for years.

What sarcopenia is
Sarcopenia is the progressive age-related loss of muscle mass, strength, and function. The term was introduced by Irwin Rosenberg in 1989 and has since become a standard diagnostic concept in geriatrics and sports medicine. According to the European Working Group on Sarcopenia in Older People (EWGSOP), diagnosis requires concurrent reduction in muscle strength, mass, and physical performance.
Prevalence is significant: sarcopenia is diagnosed in one in five people over 65 and one in two over 80.
The mechanism of loss
At the cellular level, sarcopenia develops through several parallel processes. The rate of muscle protein synthesis declines — particularly myofibrillar protein responsible for contractile function. The number and cross-sectional area of type II muscle fibres — fast-twitch fibres critical for strength and power — decreases. Mitochondrial density in muscle tissue falls.
Simultaneously, denervation occurs — motor neurons lose their connection to muscle fibres. According to research by Lexell et al. published in Journal of the Neurological Sciences, by age 70 a person loses approximately 25% of motor units compared to peak values in young adulthood.
Why this matters beyond strength
Muscles are the largest metabolically active organ in the body. They absorb approximately 80% of blood glucose following a meal. With sarcopenia, this capacity declines, increasing the risk of insulin resistance and type 2 diabetes independent of body mass index.

A study published in Journal of Cachexia, Sarcopenia and Muscle found that people with low muscle mass have a 2.3 times higher risk of fractures from falls and significantly elevated metabolic disease risk. Muscles secrete myokines — cytokines with anti-inflammatory properties. Their loss affects not only mechanical function but systemic inflammation and immune response.
The only intervention with proven effectiveness
Progressive resistance training is the most studied and effective method for preventing and treating sarcopenia. Training stimulates muscle protein synthesis through activation of the mTOR signalling pathway, increases mitochondrial density, improves neuromuscular coordination, and enhances insulin sensitivity.

A meta-analysis published in the British Journal of Sports Medicine covering data from over 3,000 participants over 60 showed that progressive resistance training reliably increases muscle mass and strength at any age. The optimal protocol is 2–3 sessions per week at 70–85% of one-repetition maximum. After 12 weeks, participants over 60 showed strength gains bringing them to levels 15–20 years younger.
The principle of progressive overload is essential. The body adapts to constant load and stops responding to it with growth. Load must gradually increase.
Tracking the trend
Sarcopenia develops slowly and is subjectively almost imperceptible in its early stages. VO2 max and resting heart rate serve as indirect markers of muscular system health — metrics that reflect cardiorespiratory and muscle function together. A decline in VO2 max at stable weight and lifestyle is one signal worth paying attention to.

Arry tracks the VO2 max and resting heart rate trend from Apple Health data — so you see the direction over months, not just today's number. arry.app
Sources
- Cruz-Jentoft AJ, et al. (2019) — Sarcopenia: revised European consensus on definition and diagnosis. Age and Ageing.
- Ethgen O, et al. (2017) — The Future Prevalence of Sarcopenia in Europe. Gerontology.
- Lexell J, Taylor CC, Sjöström M. (1988) — What is the cause of the ageing atrophy? Journal of the Neurological Sciences.
- Beaudart C, et al. (2016) — Sarcopenia in daily practice: assessment and management. BMC Geriatrics.
- Liao CD, et al. (2017) — Effects of resistance training in elderly with sarcopenia. British Journal of Sports Medicine.